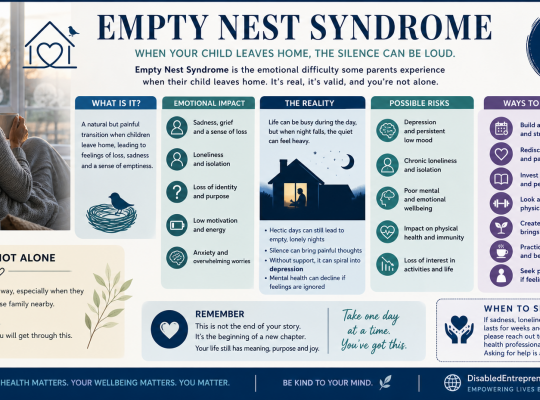
Empty Nest Syndrome: When Silence Feels Loudest
A compassionate guide to Empty Nest Syndrome, exploring its emotional impact and offering practical ways to cope with loneliness, especially for parents without partners or family support.
DISABLED ENTREPRENEUR – DISABILITY UK
Disability UK Online Health Journal – All In One Business In A Box – Forum – Business Directory – Useful Resources – Health – Human Rights – Politics
DISABLED ENTREPRENEUR – DISABILITY UK
Disability UK Online Health Journal – All In One Business In A Box – Forum – Business Directory – Useful Resources – Health – Human Rights – Politics
Browsing Category
A compassionate guide to Empty Nest Syndrome, exploring its emotional impact and offering practical ways to cope with loneliness, especially for parents without partners or family support.
A comprehensive guide to retirement, mental health, and staying active. Learn how athletes and everyday people can reinvent themselves, reduce dementia risk, and find purpose after work.

An in-depth look at depression, trauma, and PIP assessments, exploring why outward behaviour does not reflect mental health and how self-help strategies support recovery.

An in-depth legal guide on search warrants, digital tracking “pings,” and your rights when police search the wrong property. Learn about UK law, compensation, and how to challenge unlawful searches.
Many of today’s most respected shows focus on practical habits backed by neuroscience, psychology, and long-term research. By listening consistently, people can pick up realistic strategies that support brain health without drastic lifestyle changes.

Exploring psychology, human behaviour, and why healthcare professionals should avoid trigger wording when discussing mental health with patients. Learn about patient rights and UK legal protections.

Coping with grief while studying or working can be challenging, but it’s possible with the right strategies and support systems in place. By acknowledging your feelings, communicating with others, practicing self-care, setting realistic goals, seeking professional help if needed, and being patient with yourself, you can navigate through grief while still fulfilling your responsibilities and moving forward in your academic or professional pursuits.
An honest, first-person article on relationship breakups, unrequited love, divorce, and healing, offering practical guidance on what to do and what not to do when your heart is broken.

A first-person account of mental-health stigma within a traditional rural Polish family: why it’s hard to explain mental health to older generations, how judgement impacts wellbeing, and what the statistics say about stigma and discrimination in Poland.

Hoarding is a serious disorder with far-reaching consequences. Understanding its causes, recognizing its symptoms, and seeking appropriate treatment can significantly improve the lives of those affected. By increasing awareness and compassion, we can better support individuals in overcoming the challenges associated with hoarding and help them lead healthier, more organized lives.