The Connection Between Stress and Memory Loss, Can Chronic Stress Become Dangerous?
Explore how chronic stress, anxiety, grief, trauma and stonewalling can affect memory, physical health, relapses and potential legal accountability.
DISABLED ENTREPRENEUR – DISABILITY UK
Disability UK Online Health Journal – All In One Business In A Box – Forum – Business Directory – Useful Resources – Health – Human Rights – Politics
DISABLED ENTREPRENEUR – DISABILITY UK
Disability UK Online Health Journal – All In One Business In A Box – Forum – Business Directory – Useful Resources – Health – Human Rights – Politics
Browsing Category
Explore how chronic stress, anxiety, grief, trauma and stonewalling can affect memory, physical health, relapses and potential legal accountability.

Learn how disabled renters can manage maintenance visits, safety inspections and valuations, request reasonable adjustments and protect their tenant rights.
Stress can cause sleep problems, a high resting heart rate, overthinking, anxiety, bladder symptoms and worsening health conditions. This article explores how stress affects disabled people, entrepreneurs, workers and people living with trauma or autoimmune diseases such as multiple sclerosis.

An educational article exploring violence among children and teenagers, knife crime, bullying, sextortion, drugs, nitrous oxide balloons, vehicle-related violence, domestic abuse exposure, safeguarding duties and the urgent need for schools to teach young people the law and consequences of crime.

An in-depth article exploring sexual assault, rape, victim trauma, fear of not being believed, evidence gathering, whistleblowing, mental health impacts, and failures within the justice system.

Alcohol is a toxic depressant that affects the brain, body, mental health, judgment, and behaviour. Learn the dangers of alcohol misuse, recovery, brain healing, addiction, and why many successful people choose sobriety.
As the Timms Review deadline approaches, concerns grow over whether the PIP system is fit for purpose. Campaigners, disabled people, and advocacy groups call for dignity, compassion, and reform in disability assessments.

A comprehensive guide exploring the connection between OCD, trauma, grief, anxiety, financial stress, stonewalling, social isolation, and mental health deterioration, including legal rights, triggers, coping strategies, and motivational recovery advice.

An in-depth UK guide on domestic violence, children witnessing abuse, police powers to remove children, legal rights, and support for affected families.
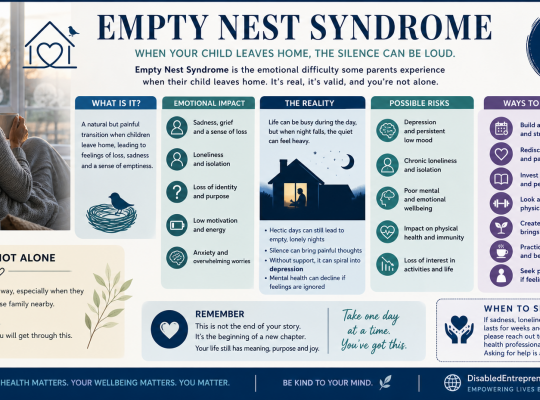
A compassionate guide to Empty Nest Syndrome, exploring its emotional impact and offering practical ways to cope with loneliness, especially for parents without partners or family support.