The Connection Between Stress and Memory Loss, Can Chronic Stress Become Dangerous?
Explore how chronic stress, anxiety, grief, trauma and stonewalling can affect memory, physical health, relapses and potential legal accountability.
DISABLED ENTREPRENEUR – DISABILITY UK
Disability UK Online Health Journal – All In One Business In A Box – Forum – Business Directory – Useful Resources – Health – Human Rights – Politics
DISABLED ENTREPRENEUR – DISABILITY UK
Disability UK Online Health Journal – All In One Business In A Box – Forum – Business Directory – Useful Resources – Health – Human Rights – Politics
Browsing Category
Explore how chronic stress, anxiety, grief, trauma and stonewalling can affect memory, physical health, relapses and potential legal accountability.
Stress can cause sleep problems, a high resting heart rate, overthinking, anxiety, bladder symptoms and worsening health conditions. This article explores how stress affects disabled people, entrepreneurs, workers and people living with trauma or autoimmune diseases such as multiple sclerosis.
Exploring antisemitism, Zionism, social unrest, and how conflict affects vulnerable people and disabled communities. Discusses empathy, emotional well-being, education, and peaceful coexistence.
A comprehensive guide to Tourette syndrome, public awareness, disability rights, UK law, the Mason airport incident, coping strategies, and how businesses can better support neurodivergent individuals.
As the Timms Review deadline approaches, concerns grow over whether the PIP system is fit for purpose. Campaigners, disabled people, and advocacy groups call for dignity, compassion, and reform in disability assessments.

A comprehensive guide exploring the connection between OCD, trauma, grief, anxiety, financial stress, stonewalling, social isolation, and mental health deterioration, including legal rights, triggers, coping strategies, and motivational recovery advice.
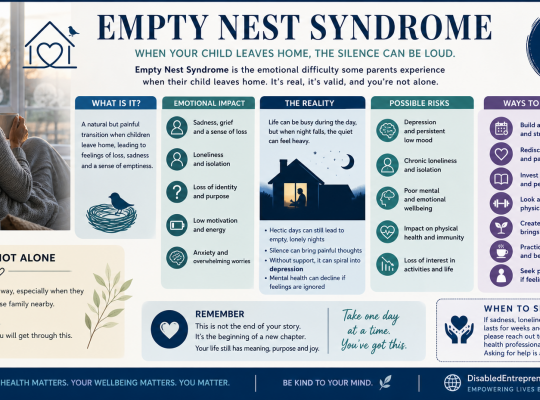
A compassionate guide to Empty Nest Syndrome, exploring its emotional impact and offering practical ways to cope with loneliness, especially for parents without partners or family support.
An insightful look into the psychology behind why people ask “How are you?” without genuine intent, and how to respond authentically while protecting your emotional well-being.

An in-depth look at depression, trauma, and PIP assessments, exploring why outward behaviour does not reflect mental health and how self-help strategies support recovery.
Learn your legal rights under UK private nuisance law, including noise complaints, barking dogs, tenant rights, and liability for street events affecting your home and work.