Cerebellar Atrophy.
Cerebellar Atrophy is something that has motivated me to do research and studies because I personally have been diagnosed with it.
My symptoms are: I lose balance and jumble my words up or miss them out completely when I speak and when I write. Thank God for ‘Grammarly.
Whilst cerebellar atrophy can be the cause of drinking heavily, I personally do not drink alcohol other than on social occasions. It can also be due to head trauma which I cannot rule out.
There is a close connection between Multiple Sclerosis (which my daughter has been diagnosed with) and Obsessive-Compulsive Disorder (which I also suffer from) as I will explain further.
What is the cerebellum and what does it do ?
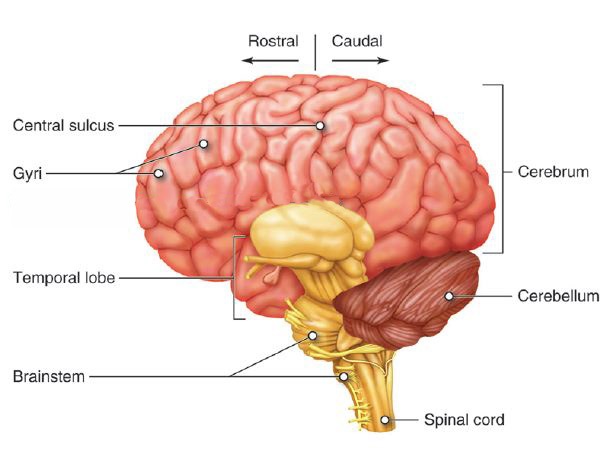
The cerebellum (“little brain”) is a structure that is located at the back of the brain, underlying the occipital and temporal lobes of the cerebral cortex. The cerebellum is involved in the following functions: Maintenance of balance and posture.
The cerebellum is part of the brain. It lies under the cerebral cortex, towards the back, behind the brainstem, and above the spinal cord. The cerebellum is largely involved in “coordination”. Persons whose cerebellum doesn’t work well are generally clumsy and unsteady. They may look like they are drunk even when they are not.
The cerebellum contains a lot of neurons. According to Hurculano-Houzel (2010), it contains about 80% of the neurons in the brain. So small in size, large in number. It must be doing something pretty important. The large neuron count probably is due to the more elaborate folding of the cerebellar cortex, as the neurons are mainly close to the periphery.
Cerebellar disorders are rare. They are often called “ataxias”. According to Musselman et al (2014), the prevalence of childhood ataxia is 26/100,000 children. Ataxia is rare compared to cerebral palsy (211/100,00) and autism (620/100,000).
Many cerebellar disorders are genetic in origin. In general, the prevalence of genetic disorders and especially autosomal recessive disorders is much higher in populations where there is more consanguinity. Examples of this include Quebec, Canada, and the Al-Kharga district in Egypt. There are also many acquired cerebellar disorders. For example, drinking too much alcohol for a long time causes a cerebellar disorder.
There are several key functions of the cerebellum, including:
- Balance and posture
- Mental function
- Movement
- Motor learning
- Vision
Causes of Cerebellum Damage
Damage to the cerebellum, or to its connection to other parts of the nervous system, can be a result of trauma, health conditions, medications, and other factors, including:
- Alcohol use disorder
- Brain tumor
- Head injury
- Huntington’s disease
- Infections
- Lead or mercury poisoning
- Medications, including benzodiazepines or barbiturates
- Multiple sclerosis
- Parkinson’s disease
- Stroke
Conditions That Affect the Cerebellum
When your cerebellum is damaged, nerve cells break down and die and can cause the following:
- Ataxia:The loss of control of voluntary movement (e.g., the ability to move your body the way you want)
- Cognitive impairment:A reduction in conscious mental activities, including thinking, learning, memory, and concentration
- Dystonia: Involuntary contraction of muscles that normally work in cooperation so that a body part is held in an unusual and often painful position as a result
- Tremors: Involuntary, rhythmic contraction of muscles that can lead to shaking movements in the hands, legs, face, head, or vocal cords
- Unsteady gait:Walking unsteadily or clumsily (A person with an unsteady gait may appear intoxicated even if that’s not the case.)
- Vertigo:The dizziness sensation of spinning, swaying, or tilting, which is frequently associated with balance problems and often accompanied by nausea, vomiting, headache, or hearing loss
Diagnosis of Cerebellar disorders
The main clinical features of cerebellar disorders include incoordination, imbalance, and troubles with stabilizing eye movements. There are two distinguishable cerebellar syndromes — midline and hemispheric.
Midline cerebellar syndromes are characterized by imbalance. Persons are unsteady, they are unable to stand in Romberg with eyes open or closed, and are unable to well perform tandem gait. Severe midline disturbance causes “trunkal ataxia” a syndrome where a person is unable to sit on their bed without steadying themselves. Some persons have “titubation” or a bobbing motion of the head or trunk. Midline cerebellar disturbances also often affect eye movements. There may be nystagmus, ocular dysmetria, and poor pursuit.
Hemispheric cerebellar syndromes are characterized by incoordination of the limbs. There may be the decomposition of movement, dysmetria, and rebound. Dysdiadochokinesis is the irregular performance of rapid alternating movements. Intention tremors may be present in an attempt to touch an object. A kinetic tremor may be present in motion. The finger-to-nose and heel-to-knee tests are classic tests of hemispheric cerebellar dysfunction. While reflexes may be depressed initially with hemispheric cerebellar syndromes, this cannot be counted on. Speech may be dysarthric, scanning, or have an irregular emphasis on syllables.
Maintenance of balance and posture. The cerebellum is important for making postural adjustments in order to maintain balance. Through its input from vestibular receptors and proprioceptors, it modulates commands to motor neurons to compensate for shifts in body position or changes in load upon muscles. Patients with cerebellar damage suffer from balance disorders, and they often develop stereotyped postural strategies to compensate for this problem (e.g., a wide-based stance).
Coordination of voluntary movements. Most movements are composed of a number of different muscle groups acting together in a temporally coordinated fashion. One major function of the cerebellum is to coordinate the timing and force of these different muscle groups to produce fluid limb or body movements.
Motor learning. The cerebellum is important for motor learning. The cerebellum plays a major role in adapting and fine-tuning motor programs to make accurate movements through a trial-and-error process (e.g., learning to hit a baseball).
Cognitive functions. Although the cerebellum is most understood in terms of its contributions to motor control, it is also involved in certain cognitive functions, such as language. Thus, like the basal ganglia, the cerebellum is historically considered as part of the motor system, but its functions extend beyond motor control in ways that are not yet well understood.
Credit:
https://nba.uth.tmc.edu/neuroscience/m/s3/chapter05.html
Cerebellar Atrophy is one of the diagnostic features in PEHO syndrome (progressive encephalopathy with edema, hypsarrhythmia, and optic atrophy) and usually appears in the second year of life.
Symptoms of Cerebellar Atrophy.
The most characteristic symptom of cerebellar degeneration is a wide-based, unsteady, lurching walk, often accompanied by a back and forth tremor in the trunk of the body. Other symptoms may include slow, unsteady, and jerky movement of the arms or legs slowed and slurred speech, dizziness, lightheadedness, loss of balance, cognitive impairment, and nystagmus.
Credit:
https://dizziness-and-balance.com/disorders/central/cerebellar/cerebellar.htm
Cerebellar atrophy in the context of other disorders
Cerebellar Atrophy is the neuroradiological hallmark of many progressive ataxias of childhood. It is a nonspecific, yet useful neuroradiological sign (Poretti et al., 2008). Its differentiation from cerebellar hypoplasia can be difficult, especially if progression cannot be proven by repeated MRI. It is defined as a structurally normal cerebellum with enlarged interfolial spaces in a posterior fossa of normal size, while in cerebellar hypoplasia, the cerebellum is small and compact, without widened fissures between the foliae. Besides the hereditary ataxias, cerebellar atrophy can also be found in a multitude of other disorders, often, but not always, with additional neuroradiological abnormalities. If cerebellar atrophy is present, ataxia is often a clinical symptom, but this is not always the case. Hyperintensity of the cerebellar cortex in T2w images has been considered as pathognomonic for infantile neuroaxonal dystrophy (INAD), but has also been demonstrated in Marinesco–Sjögren syndrome or mitochondrial disorders.
Prominent cerebellar atrophy is present in many of the neurodegenerative disorders of childhood, including metabolic disorders. It can be an isolated neuroradiological feature in juvenile GM2 gangliosidosis. In late-infantile neuronal ceroid lipofuscinosis and Niemann–Pick disease type C, it is usually accompanied by mild supratentorial atrophy. It is part of the neuroradiological abnormalities in many disorders of white matter, especially in hypomyelination of basal ganglia and cerebellum (HABC) and the 4H syndrome (hypomyelination, hypodontia, and hypogonadotropic hypogonadism). In white matter disorders, the MRI appearance of the white matter is mostly sufficiently specific to make a diagnosis. Cerebellar atrophy is one of the diagnostic features in PEHO syndrome (progressive encephalopathy with edema, hypsarrhythmia, and optic atrophy) and usually appears in the second year of life. Pontocerebellar atrophy is prominent in certain subtypes of the congenital disorders of glycosylation (CDG), especially in CDG Ia which is a differential diagnosis for pontocerebellar hypoplasia.
Cerebellar Atrophy can also be acquired. Extreme prematurity can cause pontocerebellar atrophy. Acute cerebellitis and autoimmune disorders such as opsoclonus myoclonus syndrome can lead to cerebellar atrophy. More frequent causes of cerebellar atrophy are posterior fossa surgery or radiotherapy (Poretti et al., 2008).
Cerebellar Degeneration is a condition in which cerebellar cells, otherwise known as neurons, become damaged and progressively weaken in the cerebellum. There are two types of cerebellar degeneration; paraneoplastic cerebellar degeneration, and alcoholic or nutritional cerebellar degeneration. As the cerebellum contributes to the coordination and regulation of motor activities, as well as controlling the equilibrium of the human body, any degeneration to this part of the organ can be life-threatening. Cerebellar degeneration can result in disorders in fine movement, posture, and motor learning in humans, due to a disturbance of the vestibular system. This condition may not only cause cerebellar damage on a temporary or permanent basis, but can also affect other tissues of the central nervous system, including the cerebral cortex, spinal cord, and the brainstem (made up of the medulla oblongata, midbrain, and pons).
Cerebellar Degeneration can be attributed to a plethora of hereditary and non-hereditary conditions. More commonly, cerebellar degeneration can also be classified according to conditions that an individual may acquire during their lifetime, including infectious, metabolic, autoimmune, paraneoplastic, nutritional, or toxic triggers.
Conclusions: Altered functional connectivity between the cerebellum and cerebral networks involved in cognitive-affective processing in patients with OCD provides further evidence for the involvement of the cerebellum in the pathophysiology of OCD, and is consistent with impairment in executive control and emotion
Abstract
Background: The role of the cerebellum in obsessive-compulsive disorder (OCD) has drawn increasing attention. However, the functional connectivity between the cerebellum and the cerebral cortex has not been investigated in OCD, nor has the relationship between such functional connectivity and clinical symptoms.
Methods: A total of 27 patients with OCD and 21 healthy controls (HCs) matched on age, sex and education underwent magnetic resonance imaging (MRI). Seed-based connectivity analyses were performed to examine differences in cerebellar-cerebral connectivity in patients with OCD compared with HCs. Associations between functional connectivity and clinical features in OCD were analyzed.
Results: Compared with HCs, OCD patients showed significantly decreased cerebellar-cerebral functional connectivity in executive control and emotion processing networks. Within the OCD group, decreased functional connectivity in an executive network spanning the right cerebellar Crus I and the inferior parietal lobule was positively correlated with symptom severity and decreased connectivity in an emotion processing network spanning the left cerebellar lobule VI and the lingual gyrus was negatively correlated with illness duration.
Cerebellar Atrophy & Obsessive Compulsive Disorder.
Altered functional connectivity between the cerebellum and cerebral networks involved in cognitive-affective processing in patients with OCD provides further evidence for the involvement of the cerebellum in the pathophysiology of OCD and is consistent with impairment in executive control and emotion regulation in this condition.
Keywords: Cerebellar circuits; executive control network; functional connectivity; obsessive-compulsive disorder.
Credit:
https://pubmed.ncbi.nlm.nih.gov/30058519/
Cerebellar Atrophy & Multiple Sclerosis.
Cerebellar atrophy is more extensive in patients with secondary progressive MS and those with longer disease duration when compared with people who have relapsing-remitting (RR) MS and/or shorter disease duration, and cerebellar atrophy has been shown to correlate with clinical measures of disability.
Credit:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3281565/
Credit:
https://en.wikipedia.org/wiki/Cerebellar_degeneration
#cerebellaratrophy #cerebellum #ms #ocd #multiplesclerosis #obsessivecompulsivedisorder #cerebellumatrophy

Renata The Editor of DisabledEntrepreneur.uk - DisabilityUK.co.uk - DisabilityUK.org - CMJUK.com Online Journals, suffers From OCD, Cerebellar Atrophy & Rheumatoid Arthritis. She is an Entrepreneur & Published Author, she writes content on a range of topics, including politics, current affairs, health and business. She is an advocate for Mental Health, Human Rights & Disability Discrimination.
She has embarked on studying a Bachelor of Law Degree with the goal of being a human rights lawyer.
Whilst her disabilities can be challenging she has adapted her life around her health and documents her journey online.
Disabled Entrepreneur - Disability UK Online Journal Working in Conjunction With CMJUK.com Offers Digital Marketing, Content Writing, Website Creation, SEO, and Domain Brokering.
Disabled Entrepreneur - Disability UK is an open platform that invites contributors to write articles and serves as a dynamic marketplace where a diverse range of talents and offerings can converge. This platform acts as a collaborative space where individuals or businesses can share their expertise, creativity, and products with a broader audience.