Disclaimer: This article is for informational and educational purposes only and does not constitute medical or legal advice. Readers experiencing mental health distress should seek professional support from qualified healthcare providers. If you believe a healthcare interaction has caused harm or emotional distress, you may consider raising a formal complaint through your GP practice, NHS complaints procedure, or regulatory bodies. Laws and policies referenced may change and readers should conduct their own research or seek independent legal advice.
The Psychology of Intrusive Thoughts and the Importance of Trauma-Informed Communication
Healthcare professionals play a critical role not only in treating physical illness but also in protecting the psychological wellbeing of their patients. However, communication that lacks sensitivity can unintentionally cause emotional harm, particularly for individuals who live with trauma, obsessive compulsive disorder (OCD), or intrusive thought disorders.
Questions that appear routine within clinical checklists may carry a far greater psychological impact when delivered without context, empathy, or professional judgement.
This is especially relevant when patients are asked direct questions about self-harm or suicidal thoughts during routine consultations.
While safeguarding is important, poorly delivered questioning can trigger distressing cognitive responses in vulnerable individuals.
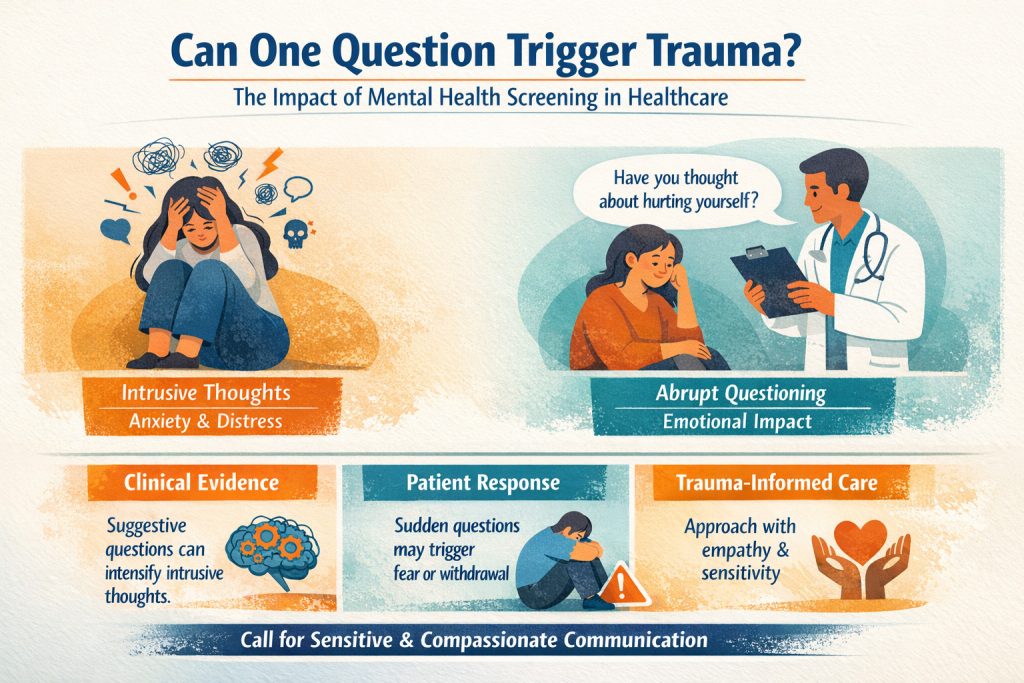
Can One Question Trigger Trauma?
Experts warn that intrusive thought disorders and trauma require more sensitive communication in clinical settings
This question sits at the heart of a growing discussion within healthcare, psychology, and patient advocacy communities.
While safeguarding questions about self-harm are intended to protect vulnerable patients, some clinicians and researchers are beginning to question whether routine or poorly contextualised mental health screening may unintentionally cause psychological distress for certain individuals.
For people living with trauma-related conditions or obsessive intrusive thought disorders such as OCD, the sudden introduction of distressing topics during routine consultations can trigger anxiety, rumination, and intrusive thought cycles.
Clinical psychology research suggests that when certain thoughts are introduced into the mind, particularly those associated with fear or danger, they can become difficult to dismiss. This phenomenon has been studied extensively in cognitive psychology and forms part of the wider understanding of how intrusive thoughts operate.
Mental health experts therefore emphasise the importance of trauma-informed communication, where healthcare professionals consider not only what questions are asked, but also how and why they are asked.
Safeguarding remains an essential responsibility within healthcare systems such as the National Health Service, and professionals are guided by ethical standards set by organisations including the General Medical Council.
However, growing awareness of trauma-informed care suggests that sensitive communication may be just as important as clinical protocols when addressing mental health concerns.
The debate is therefore not about whether patient safety questions should be asked, but about ensuring they are delivered with empathy, context, and professional judgement so that the process of safeguarding does not itself cause distress.
Understanding Intrusive Thoughts and OCD
Intrusive thoughts are unwanted, distressing thoughts that enter a person’s mind without invitation. They are commonly associated with Obsessive Compulsive Disorder (OCD) and trauma-related conditions.
According to the National Health Service, individuals with OCD may experience intrusive thoughts that are disturbing, irrational, or frightening.
These thoughts do not reflect the person’s intentions or desires, yet they can cause intense anxiety.
Ironically, the more a person tries to suppress these thoughts, the stronger they can become.
This psychological mechanism is known as the “rebound effect” in cognitive psychology.
When Healthcare Communication Causes Harm
In some cases, insensitive questioning can lead to:
- Heightened anxiety
- Increased intrusive thoughts
- Emotional distress
- Loss of trust in healthcare providers
- Deterioration in mental wellbeing
For individuals managing trauma or obsessive thought disorders, these effects can undo months, or even years, of psychological progress.
Legal Protections for Patients in the UK
Patients in the UK are not without protection when healthcare communication causes harm.
Several legal frameworks apply.
Equality and Disability Protections
Under the Equality Act 2010, healthcare providers must avoid discrimination against individuals with disabilities, including mental health conditions such as OCD or trauma-related disorders.
Healthcare providers are expected to make reasonable adjustments in how services are delivered.
Insensitive communication that disregards known vulnerabilities may raise concerns under this legislation.
The Hidden Power of Words in Healthcare
Healthcare professionals play a critical role not only in treating physical illness but also in protecting the psychological wellbeing of their patients. However, communication that lacks sensitivity can unintentionally cause emotional harm, particularly for individuals who live with trauma, obsessive compulsive disorder (OCD), or intrusive thought disorders.
Questions that appear routine within clinical checklists may carry a far greater psychological impact when delivered without context, empathy, or professional judgement.
This is especially relevant when patients are asked direct questions about self-harm or suicidal thoughts during routine consultations.
While safeguarding is important, poorly delivered questioning can trigger distressing cognitive responses in vulnerable individuals.
The Rebound Effect: Why Suggestion Matters
The rebound effect was famously demonstrated by social psychologist Daniel Wegner, whose research showed that attempting to suppress thoughts can actually make them more persistent.
In his well-known experiment, participants were instructed not to think about a white bear.
Unsurprisingly, the instruction caused participants to think about the white bear more frequently.
This phenomenon explains why certain direct questions, especially about self-harm, can unintentionally plant or reinforce distressing cognitive loops in individuals prone to intrusive thinking.
For someone already working hard to manage trauma or obsessive thought patterns, such questioning may trigger a cascade of anxiety and rumination.
Trauma-Informed Communication in Healthcare
Modern healthcare increasingly recognises the importance of trauma-informed care.
Trauma-informed communication means understanding that many patients carry unseen psychological burdens and that certain questions or phrases can re-activate painful memories.
Rather than blunt questioning, trauma-informed practitioners often use gentler, contextual approaches, such as:
- Asking patients how they are coping generally.
- Offering the opportunity to discuss emotional wellbeing rather than demanding disclosure.
- Allowing patients control over what they choose to share.
- Avoiding sudden or alarming questions unless clinically necessary.
This approach helps protect patients from feeling interrogated, humiliated, or coerced into discussing deeply personal experiences.
Duty of Care
Healthcare providers also owe patients a professional duty of care under UK medical law.
Professional standards set by the General Medical Council require clinicians to:
- treat patients with dignity and respect
- communicate sensitively
- consider patients’ psychological wellbeing
Failure to do so may raise professional conduct concerns.
Patient Rights within the NHS
The NHS Constitution for England states that patients have the right to be treated with respect, compassion and dignity.
This includes the expectation that healthcare professionals communicate appropriately and consider the emotional impact of their interactions.
What Patients Can Do If a GP Practice Causes Emotional Distress
If a patient believes a healthcare interaction has caused emotional harm, they may take several steps.
1️⃣ Raise the issue with the GP practice directly
Most complaints are first handled through the practice’s internal complaints procedure.
2️⃣ Request a copy of consultation records or audio recordings
Patients are entitled to access their records under UK data protection laws.
3️⃣ Escalate the complaint if necessary
If the practice response is unsatisfactory, the complaint may be escalated to the Parliamentary and Health Service Ombudsman.
4️⃣ Report professional conduct concerns
Serious communication failures can be reported to the General Medical Council.
5️⃣ Seek independent advice
Organisations such as patient advocacy groups or legal professionals may assist with complex complaints.
A Call for Compassionate Healthcare
Most healthcare professionals enter their profession with the genuine desire to help people. However, systems and checklists must never replace human empathy and professional judgement.
Words matter.
For someone fighting daily battles with trauma, anxiety, or intrusive thoughts, a single poorly delivered question can have a lasting impact.
Healthcare must strive not only to treat illness, but also to protect the dignity and psychological safety of every patient.
Trauma-informed communication is not simply good practice.
It is an ethical responsibility.
Clinical Evidence: How Suggestion Can Influence Intrusive Thoughts
Psychological research has long demonstrated that the human mind does not simply ignore unwanted thoughts when instructed to suppress them. In fact, attempts to suppress certain thoughts can cause them to become more persistent and intrusive.
One of the most influential studies on this phenomenon was conducted by Daniel Wegner, whose research into thought suppression introduced what is known as “ironic process theory.”
Wegner’s experiments showed that when participants were asked not to think about a specific subject, their minds repeatedly returned to the very thought they were attempting to avoid.
This research became widely known through the “white bear experiment”, where participants instructed not to think about a white bear reported thinking about it more frequently than those who were allowed to think freely.
The findings demonstrate that directly introducing a concept into someone’s mind, especially one associated with fear, danger, or distress, can unintentionally reinforce cognitive focus on that subject.
Clinical Research on OCD and Intrusive Thoughts
Intrusive thoughts are a core symptom of Obsessive Compulsive Disorder (OCD) and are widely documented in psychiatric research.
According to the National Institute of Mental Health, intrusive thoughts experienced by individuals with OCD can involve disturbing or unwanted themes that the person does not wish to act upon.
Importantly, individuals with OCD often experience intense anxiety because they misinterpret the presence of a thought as meaningful or dangerous, even though the thought itself is involuntary.
Research published in cognitive behavioural psychology literature has shown that attempts to control, suppress, or eliminate intrusive thoughts can paradoxically make them stronger and more persistent.
This creates a cycle where:
- A distressing thought appears.
- The individual attempts to suppress or neutralise it.
- The effort to suppress the thought increases its frequency.
This cycle is one reason why many OCD treatment approaches focus not on eliminating thoughts, but on reducing the emotional significance attached to them.
Why Context Matters in Mental Health Questioning
Clinical guidelines increasingly recognise that mental health questioning must be delivered within an appropriate clinical context.
Safeguarding questions about self-harm can be important when a patient presents with symptoms suggesting emotional distress or risk. However, psychological literature suggests that abrupt or poorly contextualised questioning may cause distress in patients who were not previously experiencing those thoughts.
For individuals already managing trauma or obsessive thinking patterns, such questions may inadvertently trigger rumination or intrusive mental loops.
This does not mean healthcare professionals should avoid safeguarding conversations entirely. Rather, it highlights the importance of trauma-informed communication, where clinicians carefully consider:
- the reason the question is being asked
- the patient’s known mental health background
- the manner in which the question is introduced
- whether the patient feels safe and supported during the conversation
When these elements are absent, even well-intentioned questions can have unintended psychological consequences.
The Importance of Trauma-Informed Practice
Modern healthcare increasingly promotes trauma-informed care, which recognises that many patients carry past experiences of psychological trauma.
A trauma-informed approach encourages healthcare professionals to prioritise:
- empathy
- patient autonomy
- respectful communication
- psychological safety
The goal is not simply to identify risk, but to ensure that the process of assessment itself does not cause additional harm.
Healthcare communication should therefore balance safeguarding responsibilities with a clear awareness that words have psychological impact.
The Ethical Debate Around Suicide Screening in Healthcare
Suicide prevention remains a critical priority within modern healthcare systems. Medical professionals are trained to identify potential warning signs and intervene early when a patient may be at risk.
In the UK, safeguarding responsibilities are guided by professional standards issued by the General Medical Council, which emphasise that healthcare professionals must take reasonable steps to protect patients whose safety may be at risk.
For this reason, many clinical checklists and medication reviews include standardised questions designed to identify potential suicidal ideation.
Supporters of routine screening argue that asking these questions directly can help identify individuals who may otherwise remain silent about their struggles. Early detection may allow healthcare providers to intervene before a crisis occurs. However, this approach has also generated debate within psychological and psychiatric communities.
Some clinicians and researchers argue that context and delivery are just as important as the question itself. When screening questions are asked abruptly or without clear clinical reasoning, patients may feel:
- Alarmed
- Confused
- Stigmatised
- Psychologically distressed
For individuals managing trauma, anxiety disorders, or obsessive intrusive thoughts, direct questioning may inadvertently trigger rumination or emotional distress rather than providing reassurance. This has led to increasing calls for trauma-informed screening approaches, where clinicians introduce sensitive topics more gradually and explain why certain questions are being asked.
Rather than appearing as an interrogation, the conversation becomes part of a supportive dialogue centred on the patient’s wellbeing.
Healthcare ethics therefore requires a careful balance between two important responsibilities:
Protecting patients who may be at risk of self-harm
Many experts believe the solution lies not in removing safeguarding questions entirely, but in improving communication training for healthcare professionals.
Sensitive questioning, appropriate context, and patient-centred communication can allow clinicians to assess risk while maintaining trust and psychological safety.
Understanding the Root Causes of Distress: Another important aspect of trauma-informed care is understanding the underlying causes of a patient’s distress before medication is prescribed. Many individuals seeking help for anxiety, depression, or intrusive thoughts may have experienced significant life events or long-term trauma that has shaped their mental wellbeing. However, in busy healthcare settings these experiences are not always explored in depth.
A more holistic approach could involve inviting patients to share, at their own pace, what factors may have contributed to their emotional difficulties in the first place. Simple screening questionnaires or gentle conversations about life experiences, stressors, and personal history may help clinicians gain a clearer understanding of a patient’s situation. This does not require patients to disclose painful details they are not ready to discuss, but it allows healthcare professionals to recognise that medication alone may not address the root causes of distress.
When clinicians understand the broader context of a patient’s life experiences, they are better equipped to offer appropriate support, whether that involves medication, therapy, lifestyle interventions, or referral to specialist services. A patient who feels heard and understood is also more likely to trust the treatment process and engage positively with their care.
Conclusion
Mental health conversations are among the most delicate interactions in healthcare. While safeguarding questions may be well-intentioned, the way they are delivered can have profound psychological effects on vulnerable patients. Clinical evidence shows that intrusive thoughts and trauma responses can be intensified when distressing ideas are introduced without context or sensitivity. For individuals working hard to overcome trauma or manage conditions such as obsessive compulsive disorder, poorly timed or abrupt questioning may undo significant emotional progress.
Not every patient will feel comfortable discussing deeply personal experiences with a healthcare professional they have only just met or spoken with, over a phone call. For individuals who are working hard to move beyond past trauma, being asked direct or abrupt questions about distressing topics can cause them to withdraw rather than open up. In many cases, a person who does not wish to relive painful experiences will simply shut down the conversation altogether.
A more compassionate approach may involve allowing the patient to guide the discussion at their own pace. Healthcare professionals could begin with broader, supportive questions such as whether the patient feels comfortable discussing their emotional wellbeing, how they have been feeling recently, or whether they have been able to manage their mental health over time. Gentle conversation about coping strategies, such as meditation, journaling, art therapy, hypnosis, spending time in nature, or other forms of self-care, may help create a safer space for dialogue.
By approaching mental health conversations gradually and respectfully, clinicians can reduce the risk of patients feeling pressured, overwhelmed, or retraumatised. Patients who feel safe and respected are far more likely to engage openly than those who feel confronted with questions that force them to revisit painful memories. Healthcare systems must therefore ensure that safeguarding practices are paired with trauma-informed communication training, allowing professionals to protect patients without unintentionally causing harm. Ultimately, compassionate communication is not simply good bedside manner, it is a core component of safe and ethical healthcare.
“Sometimes the most important question in healthcare is not what we ask, but how and when we ask it.”
Further Reading & Resources
- https://willproject.org/history/biographies/daniel-wegner/
- https://www.gmc-uk.org/
- https://disabledentrepreneur.uk/the-psychology-of-language-in-healthcare/
- https://disabledentrepreneur.uk/living-with-trauma-the-hidden-battle-behind-mental-health-struggles/
- https://disabledentrepreneur.uk/link-between-trauma-ms-financial-stability-ocd/
- Clinical dimensions of people with co-occurring obsessive-compulsive and multiple sclerosis: | BMJ
- · OCD and Multiple Sclerosis: Causes and Connections
- · The link between money and mental health
- · Trauma-related obsessive–compulsive disorder: a review – PMC
- · OCD and Money Problems: Is There A Link? | Psych Central
- · https://www.mind.org.uk/information-support/tips-for-everyday-living/money-and-mental-health/the-link-between-money-and-mental-health/
- · https://www.harvardmagazine.com/2021/04/right-now-linking-mental-fiscal-health
- · (PDF) Financial Wellbeing and Mental Health: A Systematic Review
- · Understanding the Mental-Financial Health Connection – Financial Health Network
- · https://disabledentrepreneur.uk/?s=trauma (215 articles)
- · https://disabledentrepreneur.uk/?s=ocd (254 articles)

Renata The Editor of DisabledEntrepreneur.uk - DisabilityUK.co.uk - DisabilityUK.org - CMJUK.com Online Journals, suffers From OCD, Cerebellar Atrophy & Rheumatoid Arthritis. She is an Entrepreneur & Published Author, she writes content on a range of topics, including politics, current affairs, health and business. She is an advocate for Mental Health, Human Rights & Disability Discrimination.
She has embarked on studying a Bachelor of Law Degree with the goal of being a human rights lawyer.
Whilst her disabilities can be challenging she has adapted her life around her health and documents her journey online.
Disabled Entrepreneur - Disability UK Online Journal Working in Conjunction With CMJUK.com Offers Digital Marketing, Content Writing, Website Creation, SEO, and Domain Brokering.
Disabled Entrepreneur - Disability UK is an open platform that invites contributors to write articles and serves as a dynamic marketplace where a diverse range of talents and offerings can converge. This platform acts as a collaborative space where individuals or businesses can share their expertise, creativity, and products with a broader audience.